Rezep
Adept
Leaked Conspiracy Theory behind Coronil
The cause is a lot simpler than you thinkWell, when we ventilate patients, we are accused of being using mechanical ventilation too early. When we wait, and the patient dies, it is complete lack of critical care. I agree, in some cases in India, there is lack of critical care, BUT many patients in Europe/US actually died with best possible critical care set ups. I personally put a young patient through ECMO for 12 days. We were supporting everything ( ventilation/dialysis/ vasopressors/ECMO) yet he died of a massive posterior circulation stroke ( I do not know of any critical care facility which can take care of ponto-medullary functions from outside)
People are dying because we do not have a cure for this virus.
Let me tell you one thing ( uncle Google won`t be able to tell you this) Critical Care medicine is basically extremely glorified symptomatic management ( other than bacterial sepsis few cardiac emergencies, very few neurological emergencies)
I/ we/ 56incher do not decide the timeline buddy, it is the damn virus who does. And sadly for India, it now has a vast susceptible population to infect and kill and unfortunately India can not go back to lockdown when this thing peaks.
Post automatically merged:
This is Czech Republic's site where anyone can enter and look for any statistical data.
COVID-19 | Onemocnění Aktuálně MZČR
Onemocnění COVID-19 je způsobeno novým typem koronaviru s odborným označením SARS-CoV-2. Vysoceinfekční onemocnění, které se projevuje zejména horečkami, respiračními potížemi (kašel, dušnost), bolestí svalů a únavou.onemocneni-aktualne.mzcr.cz
Anyone can request for the raw data, they are not hiding anything.
Please use Google translate if don't read Czech.

The cause is a lot simpler than you think
Read the high courts judgement
They compare two hospitals with very different results. Why is that difference there ?
Same thing is happening in LNJP Delhi
This is complete mismanagement. There was enough time to allocate resources. These are not backward states. There is no shortage of personnel.
View attachment 86529
Compare infrastructure between TN & Maha. Same isn't it. Look at the difference in death rates.
Why is it 10x higher for Maha, all other things being equal ?
This is a very controllable disease if you have an adminstration that wants to do it.
This is a very controllable disease if you have an adminstration that wants to do it.

Dear, I have no idea about your experience and competency in critical care. We treat patients with our knowledge, skill sets and personal experience, not some court order. Yes, sure it is a very controllable disease yet we do not yet know the exact mode of transmission, range of incubation period, even all the symptoms.The cause is a lot simpler than you think
Read the high courts judgement
They compare two hospitals with very different results. Why is that difference there ?
Same thing is happening in LNJP Delhi
This is complete mismanagement. There was enough time to allocate resources. These are not backward states. There is no shortage of personnel.
View attachment 86529
Compare infrastructure between TN & Maha. Same isn't it. Look at the difference in death rates.
Why is it 10x higher for Maha, all other things being equal ?
This is a very controllable disease if you have an adminstration that wants to do it.

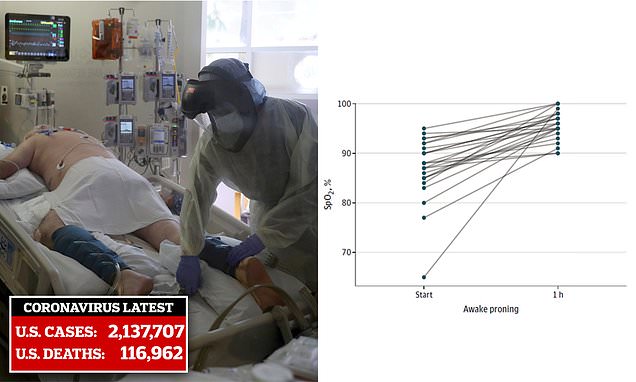
In non ventilated patients, nope, but used prone ventilation in lot of patients.
The study is interesting. Wondering how did they turn a severely dyspneic patient to prone position without putting in an ET tube.
I mean, if you put a dyspneic patient prone and if he/ she worsens, how the hell are you going to intubate in prone position?
 mobile.reuters.com
mobile.reuters.com
You seem to know this inside and out, must be keeping tabs on the developing situation with hydroxychloroquine? Apparently it actually does work to some degree according to recent studies. What do you make of it?Throughout the interview Mr. Trivedi failed to understand a single question and spewed the same nonsense over and over again!! It was really painful to go through the entire video.
This thing enters CNS through cribriform plate ( causing damage to olfactory nerve leading to anosmia) however it causes selective vasculitis of the posterior circulation!!
...
